Appointments
01733 842 309
Email Secretary




Arthroscopy of the Knee
The information contained within this leaflet is only a guide and the timings and activities will depend upon your specific circumstances and the surgeon's individual requirements.
The booklet has been designed to help you understand and recover from your arthroscopy. An arthroscopy (looking inside a joint with a special 'camera-type' instrument) is a surgical technique that allows your orthopaedic surgeon to see clearly inside your knee in order to treat the problem where possible.
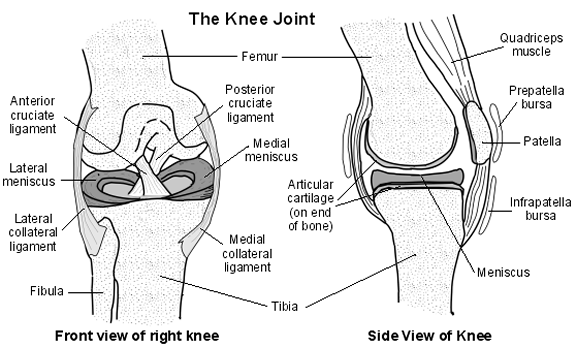
The knee is a hinge joint. It is formed by the lower end of the thigh bone (femur), the top of the shinbone (tibia) and the patella (kneecap), which sits in front of the knee. In a healthy joint the bone ends and the underside of the kneecap (patella) are covered by articular cartilage, which allows the bones to glide easily against each other. Cartilage does not contain any nerves and therefore the movement is pain free. There is also another type of cartilage called the meniscus. There are two of these in the knee joint. The menisci act as shock absorbers between the two leg bones. The ligaments, tendons and muscle provide the stability and strength to the joint.
This is a front and side view of your knee. The drawing shows the bones, ligaments and the cartilages that make up your knee.
You may be asked to attend the hospital during the two weeks prior to your operation for a general health check. Alternatively, this health check may be undertaken over the phone.
If you are asked to come to the hospital please bring an up to date list of any present medication, this can be obtained from you GP.
It is essential that you are in the best of health possible to reduce the risks from having an anaesthetic and to help with your recovery. It is very important that you prepare yourself for surgery as best you can. If you are unwell at any stage prior to surgery, call your Consultants secretary to discuss further.
Your surgery can usually be done as a day case. This means that you come into hospital on the day of your operation and can go home on the same day.
The anaesthetist will discuss the anaesthetic options available to you, this will be either general anaesthetic or spinal (epidural) anaesthetic. Once the decision on which anaesthetic will most suit you, the anaesthetist will either help you to sleep with a general anaesthetic via an injection in the back of your hand, or perform the spinal (epidural) anaesthetic which will numb you from the waist down. The operation involves two, occasionally three, small incisions (cuts) into the front of the knee joint below the knee cap. Through the incisions a telescopic camera and instruments are put into the knee joint to allow the surgeon to see and treat a variety
There are several ways of investigating knee joint problems, but arthroscopy is the only method that gives a direct view of the inside of the joint.
- Torn cartilage (Meniscus)
- Ruptured/torn anterior cruciate ligament
- Articular cartilage wear and tear (arthritic changes/ loose bodies)
- Anterior knee pain (patella)
If you have a torn meniscus (cartilage) the surgeon may remove the torn part or, in certain cases, may try and repair it.
If you have a torn ligament, the surgeon will not usually replace it during the first operation. Possible treatments will be discussed after your arthroscopy.
If the surgeon finds a loose body this will be removed through the small cuts.
If you have arthritis the surgeon will wash the joint out with a saline, which can improve your symptoms for some months. However, the arthritis will remain and take its own course.
If you have patella symptoms, they may be due to tight soft tissue on the outside of your knee joint. These tissues may be cut to release them, this is known as a lateral release.
Following surgery the cuts will be usually left open to heal naturally. Your knee will then be wrapped in wool covered by a crepe bandage.
In some cases it may be necessary to put a drain in the knee, which allows excess fluid e.g. blood, to drain off your knee. This will be removed the day following surgery, and will require you to stay in hospital overnight.
With all surgery there is a risk of complications.
- Wound infection - if the wound or directly surrounding areas become red, inflamed, painful or start weeping, consult your GP.
- Blood clots - surgery to the leg can sometimes cause a clot to form in the veins. To prevent this keep moving your legs and practice the exercises on page 10 of this leaflet.
Please discuss these issues with the medical team if you would like further information.
On return from theatre you will be encouraged to move the knee as much as comfort and the dressings allow.
You will already have been given a walking aid (usually crutches) before the operation. You will be able to walk normally unless instructed otherwise by your physiotherapist, who will decide how much you need to use any walking aid.
You should only require crutches for 2-3 days. Crutches issued must be returned to the Physiotherapy Department at Edith Cavell Hospital or the Physiotherapy Department at Peterborough District Hospital.
Once safely mobile you will be allowed home, usually three or four hours after operation. You will need to be driven home. (If possible, please arrange for a friend or relative to collect you), and have a responsible adult (friend or relative) at home with you for the first one to two days Occasionally you may have to spend one night in hospital.
The heavy bandage dressing will usually require removal at 48 hours post op. If you are still in hospital this will be done on the ward. If you have been discharged you may do this yourself or organise an appointment with the nurse at your GP practice when you leave hospital. You will be given dressings on discharge to keep the ports covered until review in the outpatient clinic. You will be given a form to hand to the practice nurse.
Once the crepe bandage has been removed you may shower getting the wound wet, however, you should avoid soaking the wound for the first week. After washing, pat dry carefully.
It is not uncommon for your knee joint to be swollen following an arthroscopy. To reduce swelling elevate your leg on a pillow and do not excessively dangle your leg for long periods in the first few days. If your knee becomes swollen, an ice pack may help. Ice packs should be applied for 20 minutes after exercise to help relieve pain.
- Soak a towelling bag or pillow case in cold water and wring out
- Place ice cubes in this and crush (alternatively, a 1lb pack of frozen peas placed in a wet towel or bag can be used)
- Make into a parcel and place on the swollen area for up to 20 minutes. The skin will then be pink.
- Do not let any unwrapped ice come into contact with the skin as this will cause an ice burn.
Repeat this 2 or 3 times a day until the swelling has subsided.
You will be given analgesia to take home. It is advisable to take this for the first 2-3 days post op, and then as you feel more comfortable reduce the frequency of taking it.
You should not attempt to drive until you feel confident to carry out a full emergency stop procedure and able to walk without stick/crutch and without limping. This will be at least 7-10 days post op on average.
This depends on the nature of your job. If you have a sedentary occupation (mainly sitting down) then on average most people will go back to work within 1-2 weeks. Those who work in more strenuous occupations may require 2-4 weeks off work. Your consultant or physiotherapist will advise you.
You may return to light gentle exercise, such as swimming or light gym work, at approximately 2 weeks post op. If you wish to go swimming, you need to wait for your wounds to heal fully before starting.
This depends on the sport you wish to return to and the surgery that has been performed. Ask your physiotherapist or consultant for advice. However, you should not run for 4-6 weeks post op.
NB - If you experience bleeding from the wound sites or develop swelling or pain in the calf following exercise, contact your GP.
Exercise is important to ensure a successful and full recovery. Strengthening the muscles (quadriceps & hamstrings) which support the knee and improving your joint mobility will ensure joint function is regained. The following exercise regime can be carried out by all patients and does not require any specialist equipment or professional assistance.
As soon as you awaken you can begin to move your feet, this assists the circulation of the blood in the legs and helps to prevent blood clots.
It is advised that you carry out these exercises for 10 minutes 3-4 times after your operation a day for at least 2 weeks.

Steps and Stairs
Always use your walking aids to support your operated leg
Going Up
- Use the hand rail withone hand
- Good leg first
- Operated leg next
- Then stick/crutch
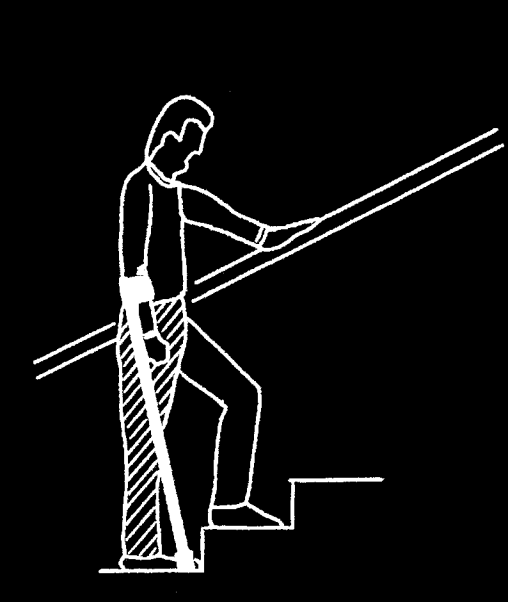
Going Down
- Crutches/Stick first
- Operated leg next
- Followed by the good leg

Specific Exercises
If you have been diagnosed with arthritis or have generalised problems you should work on all exercises.
If you have anterior knee pain (chondromalcia) or have had a lateral release, you should concentrate on quadriceps exercises. You should ask your physiotherapist to explain VMO exercises; these are specific quadriceps exercises.
If you have an anterior cruciate ligament tear you should concentrate on hamstring exercises.
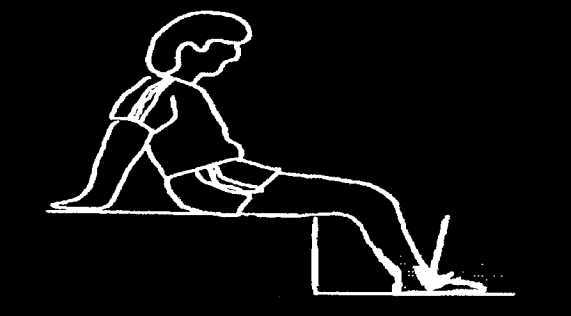
Quadriceps Sets

Sitting on the floor or the bed with your operated leg straight and your opposite knee bent.
Tighten your front thigh muscles by pressing your knee towards the floor. Hold for 6 seconds and then relax.
Knee Bending
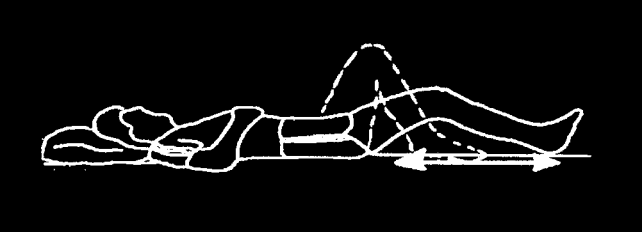
Lying flat, slide your heel towards your bottom as far as you can, hold for a few seconds and then slide back down until you knee is straight again.
After a few days this exercise can be performed whilst sitting in a chair and sliding your foot on the ground as far back under the chair as possible.
Co-Contraction (Quadriceps & Hamstrings together)
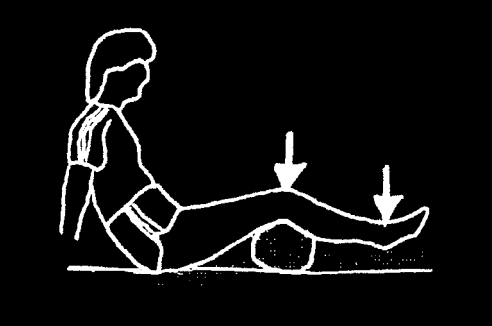
Place a rolled up towel under your knee. Push your heel and knee down into the floor at the same time. You should feel both the muscles at the front and the back of your thighs working and tight. Hold the contraction for 6 seconds and relax.
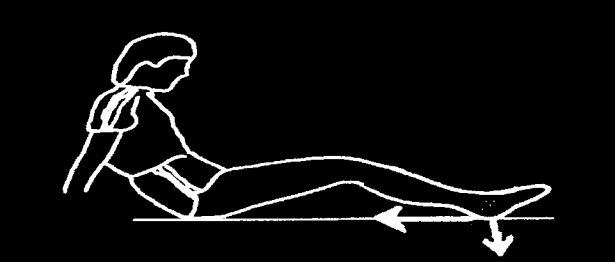
Static Hamstrings
Sitting on the floor or bed with legs out straight, bend operated leg up about 30 degrees. Push your heel hard into the floor and pull it towards your bottom without bending or moving your leg any distance. Hold for 6 seconds.
The exercise can also be performed whilst sitting in a chair. Bend your knee 60 degrees, hold onto the chair and push your heel into the floor, your knee should not move, hold for 6 seconds and relax.